by Culley C. Carson III, MD
Hypogonadism is defined as deficient or absent male gonadal function that results in insufficient testosterone secretion. Hypogonadism may be primary due to testicular failure, or secondary due to hypothalamic-pituitary axis dysfunction, resulting in the production or release of insufficient testosterone to maintain testosterone-dependent functions and systems. Hypogonadism can also result from a combination of testicular failure and hypothalamic-pituitary axis dysfunction.
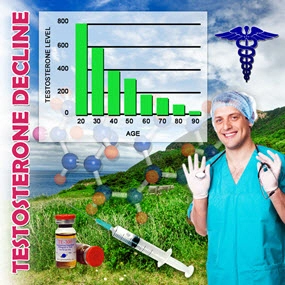
Hypogonadism affects an estimated 4 to 5 million men in the United States, and although it may occur in men at any age, low testosterone levels are especially common in older males. More than 60% of men over age 65 have free testosterone levels below the normal values of men aged 30 to 35. Studies suggest that hypogonadism in adult men is often underdiagnosed and under treated. This may be because the symptoms are easily attributed to aging or other medical causes, or ignored by patients and physicians. In fact, only about 5% of hypogonadal men receive testosterone replacement. Some experts also believe that we need to reevaluate normal testosterone the levels and lower the diagnostic cutoff for hypogonadism. By doing so, many patients who we now consider to be low- normal would probably be considered candidates for androgen replacement.
Signs and Symptoms of Hypogonadism Low testosterone, or male hypogonadism, is associated with a number of signs and symptoms, most notably loss of libido and erectile dysfunction (ED). Other signs of low testosterone include depressive symptoms, a decrease in cognitive abilities, irritability and lethargy or loss of energy. Deficient endogenous testosterone also has negative effects on bone mass and is a significant risk factor for osteoporosis in men. Progressive decrease in muscle mass and muscle strength and testicular dysfunction, often resulting in impaired sperm production, are also associated with low testosterone levels.
A younger patient may have pure hypogonadism as a primary event, whereas an older man may have an age-related decline in testosterone production that is a part of his ED profile. However, because both ED and loss of libido are hallmarks of hypogonadism, any patient who presents with ED should have a basic hormone profile to determine if he has low testosterone. Treatments to normalize testosterone can not only improve libido, energy level and the potential to have normal erections, but can also improve the response to sildenafil, if that is deemed appropriate treatment.
Screening for Hypogonadism An inexpensive and reliable screening test for hypogonadism is a morning serum total testosterone level, which measures free testosterone plus protein-bound testosterone. A morning sample is recommended, because testosterone levels demonstrate a diurnal pattern in which the highest level is reached in the early morning hours. Morning testosterone values <300 ng/dL (10.4 nmol/L) suggest hypogonadism and should be confirmed by a second assay.
If a repeat assay confirms low testosterone, luteinizing hormone (LH) should be measured to determine whether the cause is primary or secondary. LH levels <2 ng/mL suggest a hypothalamic lesion (pituitary adenoma, trauma, etc), whereas LH levels >10 ng/mL indicate primary testicular failure. Levels within the normal range suggest an age-related, decreased hypothalamic response to declining testosterone levels. In addition, serum prolactin should also be measured to rule out the presence of a pituitary tumor.
At our institution we are also currently measuring dehydroepiandrosterone (DHEA) and dehydroepiandrosterone sulfate (DHEAS) levels. Some investigators believe that replacing DHEA in patients with low libidos and normal or borderline testosterone is an important component of treatment to restore sexual desire and performance. Although controlled clinical studies are needed to confirm this approach, there is growing evidence that DHEA may play an important role in the treatment of male sexual dysfunction.
ADAM Questionnaire In addition to laboratory tests and a careful physical examination, a brief screening instrument has also been developed to aid in the diagnosis of hypogonadism. Researchers at St. Louis University created the Androgen Deficiency in the Aging Male (ADAM) questionnaire, which has been shown to be a highly sensitive (88%) instrument but with low specificity (66%), largely due to questions that identify patients with depression. However, because many men with hypogonadism dont seek medical attention, instruments such as the ADAM questionnaire can be a useful way to screen for clinical symptoms of androgen deficiency. Once testosterone deficiency is confirmed, we then consider testosterone replacement therapy.
Goals of Treatment The goal of testosterone replacement therapy is to provide and maintain a normal level of testosterone, thereby restoring libido and improving erectile function; improving mood and providing a sense of well-being; decreasing fatigue; and improving lean body mass, strength and stamina. Also, because hypogonadism is the most common cause of osteoporosis in men, testosterone replacement may improve bone density to help prevent this disease and related complications.
Visit link:
Prevalence, Diagnosis and Treatment of Hypogonadism in ...
Contact Us Today For A Free Consultation

- BioSante Pharmaceuticals, Inc. to Present at BIO Investor Forum [Last Updated On: October 24th, 2015] [Originally Added On: October 9th, 2012]
- Secondary osteoporosis: More than what meets the eye! [Last Updated On: January 15th, 2018] [Originally Added On: October 10th, 2012]
- Trimel Provides Clinical and Operational Update [Last Updated On: December 2nd, 2017] [Originally Added On: October 15th, 2012]
- Obese teen boys likelier to become impotent and infertile adults [Last Updated On: December 11th, 2017] [Originally Added On: October 17th, 2012]
- Obese teen boys have up to 50 percent less testosterone than lean boys [Last Updated On: December 27th, 2017] [Originally Added On: October 17th, 2012]
- Trimel Reports Physician Market Research Results for CompleoTRT(TM) [Last Updated On: January 8th, 2018] [Originally Added On: October 24th, 2012]
- Obese teen boys likelier to turn into 'impotent' men [Last Updated On: January 19th, 2018] [Originally Added On: October 24th, 2012]
- Trimel Pharmaceuticals Corporation to Report Third Quarter 2012 Results and Host a Conference Call to Update Investors [Last Updated On: January 2nd, 2018] [Originally Added On: November 2nd, 2012]
- Peer Exchange: Establishing Bone Health Clinics - Video [Last Updated On: January 10th, 2025] [Originally Added On: November 2nd, 2012]
- What is hypogonadism and how does it affect fertility? - Video [Last Updated On: January 10th, 2025] [Originally Added On: November 2nd, 2012]
- Low Testosterone in Men or Man-O-Pause - Video [Last Updated On: January 11th, 2025] [Originally Added On: November 2nd, 2012]
- Propecia (Finasteride) -- Undisclosed Mechanisms, Potential Dangers [Last Updated On: January 11th, 2025] [Originally Added On: November 2nd, 2012]
- How to Get Ripped - Why You Shouldnt Use Anabolic Steroids - Video [Last Updated On: January 12th, 2025] [Originally Added On: November 2nd, 2012]
- Future Doc: Andropause Alternatives with Dr. James Biddle Part 1 - Video [Last Updated On: January 12th, 2025] [Originally Added On: November 2nd, 2012]
- Sector Update: Healthcare - Video [Last Updated On: January 13th, 2025] [Originally Added On: November 2nd, 2012]
- Increase Testosterone Naturally With these Diet And Workout Secrets - Video [Last Updated On: January 13th, 2025] [Originally Added On: November 2nd, 2012]
- Signs And Symptoms of Hypogonadism [Last Updated On: December 29th, 2016] [Originally Added On: November 2nd, 2012]
- Auxilium and Pfizer Will Conclude Agreement on XIAPEX® EU Collaboration [Last Updated On: May 4th, 2015] [Originally Added On: November 9th, 2012]
- Repros Therapeutics Inc.(R) Reports Third Quarter 2012 Financial Results [Last Updated On: May 4th, 2015] [Originally Added On: November 14th, 2012]
- hypogonadotropic hypogonadism - Video [Last Updated On: February 5th, 2025] [Originally Added On: November 22nd, 2012]
- Research and Markets: Male Hypogonadism - Pipeline Review, H2 2012 [Last Updated On: December 7th, 2017] [Originally Added On: November 30th, 2012]
- Auxilium Pharmaceuticals, Inc. to Present At The Oppenheimer 23rd Annual Growth Conference [Last Updated On: May 4th, 2015] [Originally Added On: December 8th, 2012]
- Low Testosterone (Hypogonadism) - Part 2 - Video [Last Updated On: December 10th, 2012] [Originally Added On: December 10th, 2012]
- The National Mesothelioma Law Firm of Baron and Budd Reports on a New Drug that Could Improve the Health of ... [Last Updated On: May 4th, 2015] [Originally Added On: December 19th, 2012]
- Hypogonadism ¦ Treatment and Symptoms - Video [Last Updated On: March 7th, 2013] [Originally Added On: March 7th, 2013]
- Research and Markets: Male Hypogonadism Global Clinical Trials Review, H1, 2013 [Last Updated On: December 28th, 2017] [Originally Added On: May 1st, 2013]
- Male hypogonadism Prof Ossama Fouda - Video [Last Updated On: May 9th, 2013] [Originally Added On: May 9th, 2013]
- Hypogonadism - what should you do - Video [Last Updated On: July 2nd, 2013] [Originally Added On: July 2nd, 2013]
- Low Testosterone (Hypogonadism) - Part 3 - Video [Last Updated On: July 2nd, 2013] [Originally Added On: July 2nd, 2013]
- NURS805 Hypogonadism Lecture - Video [Last Updated On: August 16th, 2013] [Originally Added On: August 16th, 2013]
- Hypogonadism: MedlinePlus Medical Encyclopedia [Last Updated On: December 17th, 2017] [Originally Added On: November 3rd, 2013]
- Hypogonadism - Diseases & Conditions - Medscape Reference [Last Updated On: December 27th, 2017] [Originally Added On: November 10th, 2013]
- Hypogonadotropic hypogonadism - Wikipedia, the free encyclopedia [Last Updated On: January 24th, 2018] [Originally Added On: November 10th, 2013]
- Low Testosterone (Low-T) Normal Levels, Hypogonadism, Symptoms ... [Last Updated On: January 1st, 2018] [Originally Added On: November 15th, 2013]
- HYPOGONADISM - University of Dundee [Last Updated On: May 4th, 2015] [Originally Added On: November 23rd, 2013]
- FAQ - Hypogonadism - MEDICAL DIAGNOSIS AND MEDICINAL PLANTS [Last Updated On: January 27th, 2018] [Originally Added On: November 23rd, 2013]
- Hypogonadism - About.com Men's Health [Last Updated On: December 12th, 2017] [Originally Added On: December 2nd, 2013]
- Exciting medical advances using HRT [Last Updated On: May 4th, 2015] [Originally Added On: December 12th, 2013]
- Male hypogonadism: Symptoms - MayoClinic.com [Last Updated On: March 28th, 2020] [Originally Added On: December 12th, 2013]
- Audio-Digest Foundation Announces the Release of Oncology Volume 04, Issue 16: Highlights from Future Directions ... [Last Updated On: December 15th, 2013] [Originally Added On: December 15th, 2013]
- Hypogonadism - Medscape Reference [Last Updated On: January 29th, 2018] [Originally Added On: December 21st, 2013]
- Hypogonadism [Last Updated On: January 12th, 2018] [Originally Added On: December 23rd, 2013]
- Hypogonadism - HealthCentral [Last Updated On: December 14th, 2017] [Originally Added On: December 24th, 2013]
- Hypogonadism | Medscape - Latest Medical News, Clinical Trials ... [Last Updated On: December 18th, 2017] [Originally Added On: December 30th, 2013]
- Hypogonadism - SharedJourney [Last Updated On: December 19th, 2017] [Originally Added On: January 23rd, 2014]
- Study Finds Potential Heart Risks from Testosterone Therapy [Last Updated On: November 24th, 2020] [Originally Added On: February 3rd, 2014]
- Endocrine Society calls for large-scale studies to evaluate testosterone therapy risks [Last Updated On: November 18th, 2020] [Originally Added On: February 8th, 2014]
- Testosterone Therapy Not Always Good for Older Men [Last Updated On: October 3rd, 2020] [Originally Added On: February 11th, 2014]
- Hypogonadism: Types, Causes, & Symptoms Healthline [Last Updated On: December 5th, 2017] [Originally Added On: February 14th, 2014]
- Low Testosterone (Hypogonadism) in Men - Video [Last Updated On: November 7th, 2020] [Originally Added On: February 14th, 2014]
- Hypogonadism : Types, Causes, & Symptoms - Healthline [Last Updated On: January 28th, 2018] [Originally Added On: February 17th, 2014]
- Hypogonadism | Medscape - Latest Medical News, Clinical ... [Last Updated On: October 6th, 2020] [Originally Added On: February 23rd, 2014]
- Endo: FDA Oks AVEED Injection For Treatment Of Adult Men With Hypogonadism [Last Updated On: November 3rd, 2020] [Originally Added On: March 6th, 2014]
- Unit Project 1 Hypogonadotropic hypogonadism - Video [Last Updated On: November 26th, 2020] [Originally Added On: March 8th, 2014]
- Update on Endo's Product Portfolio - Analyst Blog [Last Updated On: October 17th, 2020] [Originally Added On: March 11th, 2014]
- Male hypogonadism Symptoms - Diseases and Conditions ... [Last Updated On: October 20th, 2020] [Originally Added On: April 2nd, 2014]
- Hypogonadism: Types, Causes, & Symptoms - Medical ... [Last Updated On: November 11th, 2020] [Originally Added On: April 6th, 2014]
- VLog #127 Frances Explains Hypogonadism. - Video [Last Updated On: November 4th, 2020] [Originally Added On: April 7th, 2014]
- Repros Completes Enrollment for Androxal Study - Analyst Blog [Last Updated On: October 27th, 2020] [Originally Added On: April 16th, 2014]
- Repros Therapeutics Q2 Loss a Penny Wider than Expected - Analyst Blog [Last Updated On: October 3rd, 2020] [Originally Added On: August 12th, 2014]
- Repros Reports Encouraging Late-Stage Data on Androxal - Analyst Blog [Last Updated On: October 5th, 2020] [Originally Added On: August 28th, 2014]
- Repros Therapeutics Analyst Brief Report; Androxal(R) Achieves Superiority in Top Line Analysis by Small Cap Street ... [Last Updated On: October 31st, 2020] [Originally Added On: September 30th, 2014]
- The Wall Street Journal: Repros Therapeutics shares drop on drug application setback [Last Updated On: October 22nd, 2020] [Originally Added On: October 18th, 2014]
- Apricus expands development pipeline with in-licensing of US rights for fispemifene [Last Updated On: November 21st, 2020] [Originally Added On: October 21st, 2014]
- Apricus expands development pipeline with the in-licensing of US rights for fispemifene, a phase 2b ready asset, from ... [Last Updated On: November 20th, 2020] [Originally Added On: October 21st, 2014]
- Hypogonadism No Moustache! No Beard!! [Last Updated On: November 20th, 2020] [Originally Added On: October 28th, 2014]
- Male Hypogonadism: Male Reproductive Endocrinology: Merck ... [Last Updated On: December 24th, 2017] [Originally Added On: October 28th, 2014]
- Hypogonadism Wikipedia [Last Updated On: November 10th, 2020] [Originally Added On: October 28th, 2014]
- Urology Care Foundation - Urology A-Z - Low Testosterone [Last Updated On: June 19th, 2015] [Originally Added On: November 3rd, 2014]
- Will Repros (RPRX) Miss Estimates This Earnings Season? - Analyst Blog [Last Updated On: October 11th, 2020] [Originally Added On: November 5th, 2014]
- Hypogonadism in men living with HIV - Video [Last Updated On: November 22nd, 2020] [Originally Added On: November 7th, 2014]
- Male Hypogonadism Therapeutic Pipeline Industry Review, H2 2014 - Video [Last Updated On: November 14th, 2020] [Originally Added On: November 7th, 2014]
- Testosterone Deficiency (Hypogonadism) Overview ... [Last Updated On: November 23rd, 2014] [Originally Added On: November 23rd, 2014]
- Endo to Acquire Rights to Testosterone Nasal Gel Natesto - Analyst Blog [Last Updated On: November 12th, 2020] [Originally Added On: November 26th, 2014]
- Male hypogonadism pathophysiology - Video [Last Updated On: October 31st, 2020] [Originally Added On: January 14th, 2015]
- Auxilium Announces Results from Special Meeting of Stockholders [Last Updated On: May 4th, 2015] [Originally Added On: January 28th, 2015]
- What is Hypogonadism - Symptoms and Treatment | Hormone ... [Last Updated On: January 5th, 2018] [Originally Added On: January 30th, 2015]
- Male Hypogonadism 1/28/15 - Video [Last Updated On: November 1st, 2020] [Originally Added On: January 31st, 2015]
- Male hypogonadism: symptoms, cause, treatment, risk ... [Last Updated On: November 12th, 2020] [Originally Added On: February 18th, 2015]
- Causes of secondary hypogonadism in males [Last Updated On: March 2nd, 2015] [Originally Added On: March 2nd, 2015]
Word Count: 437