Testosterone deficiency is frequently seen in both men and women with HIV. Endocrine abnormalities, which can affect testosterone production, have long been recognized as a complication of HIV since the earliest days of the pandemic (although it has generally been associated with late stage disease).
However, recent research has shown that nearly one out of every five men with HIV has documented testosterone deficiency, irrespective of CD4 count, viral load, or treatment status.
Similarly, testosterone deficiency is seen in one in four HIV-positive women, most often in the context of severe, unexplained weight loss (HIV wasting).
Testosterone is the steroid hormone which is central to the development of the testes (testicles) and prostate in men as well as the promotion of secondary male sexual characteristics (e.g., lean muscle mass, bone mass, hair growth). Testosterone is also important to women in maintaining normal muscle and bone mass, although at levels around 10% less than men.
In both men and women, testosterone is essential to a person's overall health and well-being, contributing to an individual's strength, energy levels, and libido.
By contrast, testosterone depletion is associated with:
Testosterone deficiency in men with HIV is largely associated with an endocrine abnormality called male hypogonadism in which the function of the male gonads (testes) is impaired, resulting in the diminished production of sex hormones beyond what would be expected of a man's specific age.
In the general population, hypogonadism is known to occur in about one in 25 men between the ages of 30 and 50, increasing to one in 14 between the ages of 50 to 79. By contrast, the incidence among men with HIV is as much as five times greater.
Hypogonadism can be caused by either a defect in the testes themselves (primary) or a dysfunction occurring outside of the testes (secondary). In adult males with HIV:
Hypogonadism can also be caused by childhood mumps or the abuse of anabolic steroids. HIV medications have not been shown to contribute to hypogonadism.
Hypogonadism in adult males is characterized by low serum (blood) testosterone levels, as well as one or several of following symptoms:
Diagnosis is made by measuring the amount of testosterone in the blood, of which there are three different subtypes. When a test is performed, the results will reveal both a person's total testosterone (all subtypes) and one of the three subtypes called free testosterone.
Free testosterone is simply a type of testosterone to which no protein is attached, allowing it enter cells and activate receptors that other subtypes can't. It is considered the most accurate measure of testosterone deficiency, despite representing only 2-3% of the total population. On its own, total testosterone is considered less accurate since results can appear normal if other non-free subtypes are elevated.
Testing should be performed early in the morning since levels can fluctuate by up to 20% during the course of a day. "Normal" levels are simply those within the reference range of the lab. These ranges can vary, but, for illustrative purposes, are roughly between
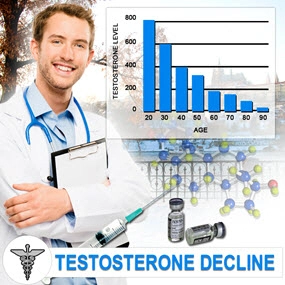
However, an assessment of "normal" cannot be made by numbers alone. Testosterone levels tend to drop by about 1-2% every year after the age of 40. Therefore, what may be "normal" for a 60-year-old male won't be the same for a 30-year-old. Assessments need to be made on an individual basis with your treating doctor.
If a diagnosis of hypogonadism is confirmed, testosterone replacement therapy may be indicated. Intramuscular testosterone injections are usually recommended, which offer low side effects if physiological doses are used and adjusted by the treating doctor. FDA-approved options include Depo-testosterone (testosterone cypionate) and Delatestryl (testosterone enanthate).
On average, injections are given every two to four weeks. To avoid the effects of fluctuating testosterone levelswhich can cause sometimes dramatic swings in mood, energy, and sexual functionlower doses and shorter dosing intervals are often used.
Side effects of treatment can include:
Testosterone replacement therapy can also cause the acceleration of pre-existing prostate cancer. Because of this, a patient's prostate-specific antigen (PSA) levels will be tested and monitored during the course of therapy.
All told, intramuscular injections offer a cost-effective option for treating hypogonadism, with associative increases in alertness, well-being, libido, lean muscle mass, and erection ability. Disadvantages include regular doctor's visits and dosing administration.
Oral, transdermal, and topical gel agents are also available, and may be applicable in certain cases. Discuss these with your doctor.
In women, testosterone is produced in the ovaries and adrenal glands. As with men, it is an important hormone for maintaining normal muscle and bone mass, as well as energy, strength, and libido.
While hypogonadism is far less common in women with HIV, it can occur and is most often in the context of HIV wasting and advanced disease. The implementation of ART can reverse wasting and the hypogonadal state in many cases.
There are currently no fixed guidelines for the treatment of female hypogonadism, and treatment options are limited. Hormone replacement therapy (HRT) may be appropriate for some, while the short-term use of testosterone may improve sex drive, lean muscle mass, and energy levels.
However, data is still incomplete on the use of testosterone to treat hypogonadism in pre-menopausal women with HIV. Speak with your health care provider about possible side effects. Testosterone is not recommended for women who are pregnant or wish to become pregnant.
Rietschel, P.; Corcoran, C.; Stanley T.; et al. "Prevalence of hypogonadism among men with weight loss related to human immunodeficiency virus infection who were receiving highly active antiretroviral therapy." Clinical Infectious Diseases. November 2, 2000; 31(5):1240-1244.
Hugh Jones, T. "Late Onset Hypogonadism." British Medical Journal. February 13, 2009; 338:b352.
Huang, J.; Wilkie, S.; Dolan, S.; et al. "Reduced testosterone levels in human immunodeficiency virus-infected women with weight loss and low weight." Clinical Infectious Diseases. January 28, 2003; 36(4):499-506.
Grinspoon, S. "The Use of Androgens in HIV-Infected Men and Women." Physicians Research Network Notebook. March 2005.
Kalyani, R.; Gavini, S.; and Dobs. A. "Male Hypogonadism in systemic disease." Endocrinology Metabolism Clinics of North America Journal. June 2007; 36(2):333-48.
Carnegie, C. "Diagnosis of Hypogonadism: Clinical Assessment and Laboratory Tests." Review in Urology. 2004; 6(6):s3-8.
Kumar, P.; Kumar, N.; Patidar, A.; et al. "Male Hypogonadism: Symptoms and treatment." Journal of Advanced Pharmacological Technology and Research. July-September 2010; 1(3): 297-302.
Mylonakis, E.; Koutkia, P.; and Grinspoon, S. "Diagnosis and treatment of androgen deficiency in human immunodeficiency virus-infected men and women." Clinical Infectious Diseases. September 15, 2001; 33(6):857-64.
Continue reading here:
HIV and Testosterone Deficiency - verywell.com
Contact Us Today For A Free Consultation

- BioSante Pharmaceuticals, Inc. to Present at BIO Investor Forum [Last Updated On: October 24th, 2015] [Originally Added On: October 9th, 2012]
- Secondary osteoporosis: More than what meets the eye! [Last Updated On: January 15th, 2018] [Originally Added On: October 10th, 2012]
- Trimel Provides Clinical and Operational Update [Last Updated On: December 2nd, 2017] [Originally Added On: October 15th, 2012]
- Obese teen boys likelier to become impotent and infertile adults [Last Updated On: December 11th, 2017] [Originally Added On: October 17th, 2012]
- Obese teen boys have up to 50 percent less testosterone than lean boys [Last Updated On: December 27th, 2017] [Originally Added On: October 17th, 2012]
- Trimel Reports Physician Market Research Results for CompleoTRT(TM) [Last Updated On: January 8th, 2018] [Originally Added On: October 24th, 2012]
- Obese teen boys likelier to turn into 'impotent' men [Last Updated On: January 19th, 2018] [Originally Added On: October 24th, 2012]
- Trimel Pharmaceuticals Corporation to Report Third Quarter 2012 Results and Host a Conference Call to Update Investors [Last Updated On: January 2nd, 2018] [Originally Added On: November 2nd, 2012]
- Peer Exchange: Establishing Bone Health Clinics - Video [Last Updated On: January 10th, 2025] [Originally Added On: November 2nd, 2012]
- What is hypogonadism and how does it affect fertility? - Video [Last Updated On: January 10th, 2025] [Originally Added On: November 2nd, 2012]
- Low Testosterone in Men or Man-O-Pause - Video [Last Updated On: January 11th, 2025] [Originally Added On: November 2nd, 2012]
- Propecia (Finasteride) -- Undisclosed Mechanisms, Potential Dangers [Last Updated On: January 11th, 2025] [Originally Added On: November 2nd, 2012]
- How to Get Ripped - Why You Shouldnt Use Anabolic Steroids - Video [Last Updated On: January 12th, 2025] [Originally Added On: November 2nd, 2012]
- Future Doc: Andropause Alternatives with Dr. James Biddle Part 1 - Video [Last Updated On: January 12th, 2025] [Originally Added On: November 2nd, 2012]
- Sector Update: Healthcare - Video [Last Updated On: January 13th, 2025] [Originally Added On: November 2nd, 2012]
- Increase Testosterone Naturally With these Diet And Workout Secrets - Video [Last Updated On: January 13th, 2025] [Originally Added On: November 2nd, 2012]
- Signs And Symptoms of Hypogonadism [Last Updated On: December 29th, 2016] [Originally Added On: November 2nd, 2012]
- Auxilium and Pfizer Will Conclude Agreement on XIAPEX® EU Collaboration [Last Updated On: May 4th, 2015] [Originally Added On: November 9th, 2012]
- Repros Therapeutics Inc.(R) Reports Third Quarter 2012 Financial Results [Last Updated On: May 4th, 2015] [Originally Added On: November 14th, 2012]
- hypogonadotropic hypogonadism - Video [Last Updated On: February 5th, 2025] [Originally Added On: November 22nd, 2012]
- Research and Markets: Male Hypogonadism - Pipeline Review, H2 2012 [Last Updated On: December 7th, 2017] [Originally Added On: November 30th, 2012]
- Auxilium Pharmaceuticals, Inc. to Present At The Oppenheimer 23rd Annual Growth Conference [Last Updated On: May 4th, 2015] [Originally Added On: December 8th, 2012]
- Low Testosterone (Hypogonadism) - Part 2 - Video [Last Updated On: December 10th, 2012] [Originally Added On: December 10th, 2012]
- The National Mesothelioma Law Firm of Baron and Budd Reports on a New Drug that Could Improve the Health of ... [Last Updated On: May 4th, 2015] [Originally Added On: December 19th, 2012]
- Hypogonadism ¦ Treatment and Symptoms - Video [Last Updated On: March 7th, 2013] [Originally Added On: March 7th, 2013]
- Research and Markets: Male Hypogonadism Global Clinical Trials Review, H1, 2013 [Last Updated On: December 28th, 2017] [Originally Added On: May 1st, 2013]
- Male hypogonadism Prof Ossama Fouda - Video [Last Updated On: May 9th, 2013] [Originally Added On: May 9th, 2013]
- Hypogonadism - what should you do - Video [Last Updated On: July 2nd, 2013] [Originally Added On: July 2nd, 2013]
- Low Testosterone (Hypogonadism) - Part 3 - Video [Last Updated On: July 2nd, 2013] [Originally Added On: July 2nd, 2013]
- NURS805 Hypogonadism Lecture - Video [Last Updated On: August 16th, 2013] [Originally Added On: August 16th, 2013]
- Hypogonadism: MedlinePlus Medical Encyclopedia [Last Updated On: December 17th, 2017] [Originally Added On: November 3rd, 2013]
- Hypogonadism - Diseases & Conditions - Medscape Reference [Last Updated On: December 27th, 2017] [Originally Added On: November 10th, 2013]
- Hypogonadotropic hypogonadism - Wikipedia, the free encyclopedia [Last Updated On: January 24th, 2018] [Originally Added On: November 10th, 2013]
- Low Testosterone (Low-T) Normal Levels, Hypogonadism, Symptoms ... [Last Updated On: January 1st, 2018] [Originally Added On: November 15th, 2013]
- HYPOGONADISM - University of Dundee [Last Updated On: May 4th, 2015] [Originally Added On: November 23rd, 2013]
- FAQ - Hypogonadism - MEDICAL DIAGNOSIS AND MEDICINAL PLANTS [Last Updated On: January 27th, 2018] [Originally Added On: November 23rd, 2013]
- Hypogonadism - About.com Men's Health [Last Updated On: December 12th, 2017] [Originally Added On: December 2nd, 2013]
- Exciting medical advances using HRT [Last Updated On: May 4th, 2015] [Originally Added On: December 12th, 2013]
- Male hypogonadism: Symptoms - MayoClinic.com [Last Updated On: March 28th, 2020] [Originally Added On: December 12th, 2013]
- Audio-Digest Foundation Announces the Release of Oncology Volume 04, Issue 16: Highlights from Future Directions ... [Last Updated On: December 15th, 2013] [Originally Added On: December 15th, 2013]
- Hypogonadism - Medscape Reference [Last Updated On: January 29th, 2018] [Originally Added On: December 21st, 2013]
- Hypogonadism [Last Updated On: January 12th, 2018] [Originally Added On: December 23rd, 2013]
- Hypogonadism - HealthCentral [Last Updated On: December 14th, 2017] [Originally Added On: December 24th, 2013]
- Hypogonadism | Medscape - Latest Medical News, Clinical Trials ... [Last Updated On: December 18th, 2017] [Originally Added On: December 30th, 2013]
- Hypogonadism - SharedJourney [Last Updated On: December 19th, 2017] [Originally Added On: January 23rd, 2014]
- Study Finds Potential Heart Risks from Testosterone Therapy [Last Updated On: November 24th, 2020] [Originally Added On: February 3rd, 2014]
- Endocrine Society calls for large-scale studies to evaluate testosterone therapy risks [Last Updated On: November 18th, 2020] [Originally Added On: February 8th, 2014]
- Testosterone Therapy Not Always Good for Older Men [Last Updated On: October 3rd, 2020] [Originally Added On: February 11th, 2014]
- Hypogonadism: Types, Causes, & Symptoms Healthline [Last Updated On: December 5th, 2017] [Originally Added On: February 14th, 2014]
- Low Testosterone (Hypogonadism) in Men - Video [Last Updated On: November 7th, 2020] [Originally Added On: February 14th, 2014]
- Hypogonadism : Types, Causes, & Symptoms - Healthline [Last Updated On: January 28th, 2018] [Originally Added On: February 17th, 2014]
- Hypogonadism | Medscape - Latest Medical News, Clinical ... [Last Updated On: October 6th, 2020] [Originally Added On: February 23rd, 2014]
- Endo: FDA Oks AVEED Injection For Treatment Of Adult Men With Hypogonadism [Last Updated On: November 3rd, 2020] [Originally Added On: March 6th, 2014]
- Unit Project 1 Hypogonadotropic hypogonadism - Video [Last Updated On: November 26th, 2020] [Originally Added On: March 8th, 2014]
- Update on Endo's Product Portfolio - Analyst Blog [Last Updated On: October 17th, 2020] [Originally Added On: March 11th, 2014]
- Male hypogonadism Symptoms - Diseases and Conditions ... [Last Updated On: October 20th, 2020] [Originally Added On: April 2nd, 2014]
- Hypogonadism: Types, Causes, & Symptoms - Medical ... [Last Updated On: November 11th, 2020] [Originally Added On: April 6th, 2014]
- VLog #127 Frances Explains Hypogonadism. - Video [Last Updated On: November 4th, 2020] [Originally Added On: April 7th, 2014]
- Repros Completes Enrollment for Androxal Study - Analyst Blog [Last Updated On: October 27th, 2020] [Originally Added On: April 16th, 2014]
- Prevalence, Diagnosis and Treatment of Hypogonadism in ... [Last Updated On: April 30th, 2014] [Originally Added On: April 30th, 2014]
- Repros Therapeutics Q2 Loss a Penny Wider than Expected - Analyst Blog [Last Updated On: October 3rd, 2020] [Originally Added On: August 12th, 2014]
- Repros Reports Encouraging Late-Stage Data on Androxal - Analyst Blog [Last Updated On: October 5th, 2020] [Originally Added On: August 28th, 2014]
- Repros Therapeutics Analyst Brief Report; Androxal(R) Achieves Superiority in Top Line Analysis by Small Cap Street ... [Last Updated On: October 31st, 2020] [Originally Added On: September 30th, 2014]
- The Wall Street Journal: Repros Therapeutics shares drop on drug application setback [Last Updated On: October 22nd, 2020] [Originally Added On: October 18th, 2014]
- Apricus expands development pipeline with in-licensing of US rights for fispemifene [Last Updated On: November 21st, 2020] [Originally Added On: October 21st, 2014]
- Apricus expands development pipeline with the in-licensing of US rights for fispemifene, a phase 2b ready asset, from ... [Last Updated On: November 20th, 2020] [Originally Added On: October 21st, 2014]
- Hypogonadism No Moustache! No Beard!! [Last Updated On: November 20th, 2020] [Originally Added On: October 28th, 2014]
- Male Hypogonadism: Male Reproductive Endocrinology: Merck ... [Last Updated On: December 24th, 2017] [Originally Added On: October 28th, 2014]
- Hypogonadism Wikipedia [Last Updated On: November 10th, 2020] [Originally Added On: October 28th, 2014]
- Urology Care Foundation - Urology A-Z - Low Testosterone [Last Updated On: June 19th, 2015] [Originally Added On: November 3rd, 2014]
- Will Repros (RPRX) Miss Estimates This Earnings Season? - Analyst Blog [Last Updated On: October 11th, 2020] [Originally Added On: November 5th, 2014]
- Hypogonadism in men living with HIV - Video [Last Updated On: November 22nd, 2020] [Originally Added On: November 7th, 2014]
- Male Hypogonadism Therapeutic Pipeline Industry Review, H2 2014 - Video [Last Updated On: November 14th, 2020] [Originally Added On: November 7th, 2014]
- Testosterone Deficiency (Hypogonadism) Overview ... [Last Updated On: November 23rd, 2014] [Originally Added On: November 23rd, 2014]
- Endo to Acquire Rights to Testosterone Nasal Gel Natesto - Analyst Blog [Last Updated On: November 12th, 2020] [Originally Added On: November 26th, 2014]
- Male hypogonadism pathophysiology - Video [Last Updated On: October 31st, 2020] [Originally Added On: January 14th, 2015]
- Auxilium Announces Results from Special Meeting of Stockholders [Last Updated On: May 4th, 2015] [Originally Added On: January 28th, 2015]
- What is Hypogonadism - Symptoms and Treatment | Hormone ... [Last Updated On: January 5th, 2018] [Originally Added On: January 30th, 2015]
- Male Hypogonadism 1/28/15 - Video [Last Updated On: November 1st, 2020] [Originally Added On: January 31st, 2015]
- Male hypogonadism: symptoms, cause, treatment, risk ... [Last Updated On: November 12th, 2020] [Originally Added On: February 18th, 2015]
Word Count: 1060